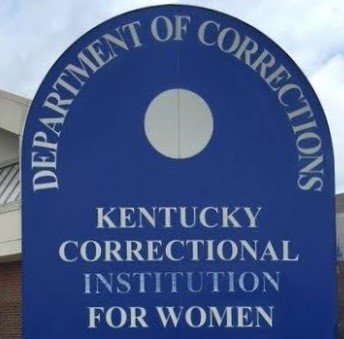
Alderson Federal Prison Camp is the oldest federal women’s prison in the United States. Founded in 1927, Alderson was meant to serve as a model of “reform”. Ten years ago, it became famous, or infamous, for housing Martha Stewart for a while. At that time, it was reputed to be one of the best prisons for women in the country. And what did that model of the best look like? “Overcrowded, understaffed, and short on funds … It now follows a punitive rather than a rehabilitative model … There’s intimidation, humiliation, and sexual harassment … a symbol of all that’s wrong with how the criminal justice system deals with women.” Ten years or so later, what’s Alderson? “Covid-19 rips through West Virginia women’s prison as federal agency takes heat”. This is the story of compassion in the covid carceral. The is the story of Rebecca “Maria” Adams, Juanita Haynes, and Bree Eberbaugh, three women who very reasonably asked for compassionate release. It never came, and, within one week in January, they died. There is no “heat” that can bring them back or bring justice for them or their loved ones.
Rebecca “Maria” Adams, Juanita Haynes, and Bree Eberbaugh’s collective list of preexisting medical conditions included Type 2 diabetes, hypertension, congestive heart failure, obesity, and chronic obstructive pulmonary disease. Any one of those should have qualified. Adams was denied. Eberbaugh was denied. Juanita Haynes was “granted release”, when she was already intubated. She died four days later. Because she died in hospital, a `free woman’, her death is not counted as a prison fatality by the Federal Bureau of Prisons. Alderson Federal Prison Camp is indeed a model, as is FCI Waseca, another low-security federal prison for women that functions as a death trap.
In March 2020, Bree Eberbaugh applied for compassionate release. In August, she was denied. The judge said the cases were too few to warrant compassionate release. As of February 8, Alderson, with fewer than 700 `residents’, reported 50 cases. Many assume the numbers of both cases, and, given what happened to Juanita Haynes, deaths is considerably higher. Eberbaugh appealed that decision. In April 2021, the appeal was denied. Nine months later, Bree Eberbaugh died.
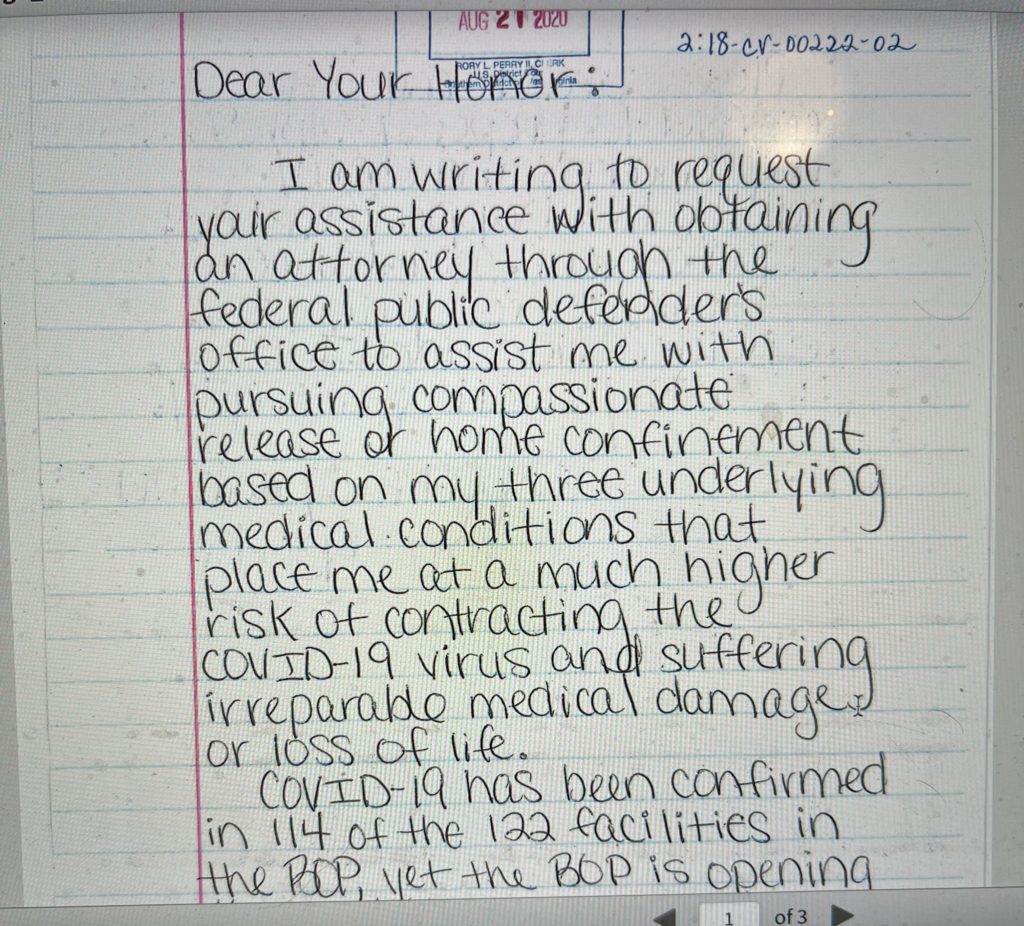
This is the text of the handwritten letter Bree Eberbaugh wrote to the judge after the first denial:
“Dear Your Honor:
I am writing to request your assistance to obtain an attorney through the federal public defender’s office to assist me with pursuing compassionate release or home confinement based on my three underlying medical conditions that place me at a much higher risk of contracting the COVID-19 virus and suffering irreparable medical damage or loss of life.
COVID-19 has been confirmed in 114 of the 122 facilities in the BOP, yet the BOP is opening the facilities up to accept transfers from other institutions. Your Honor, it is only a matter of time before it reaches here and I am in fear of my life.
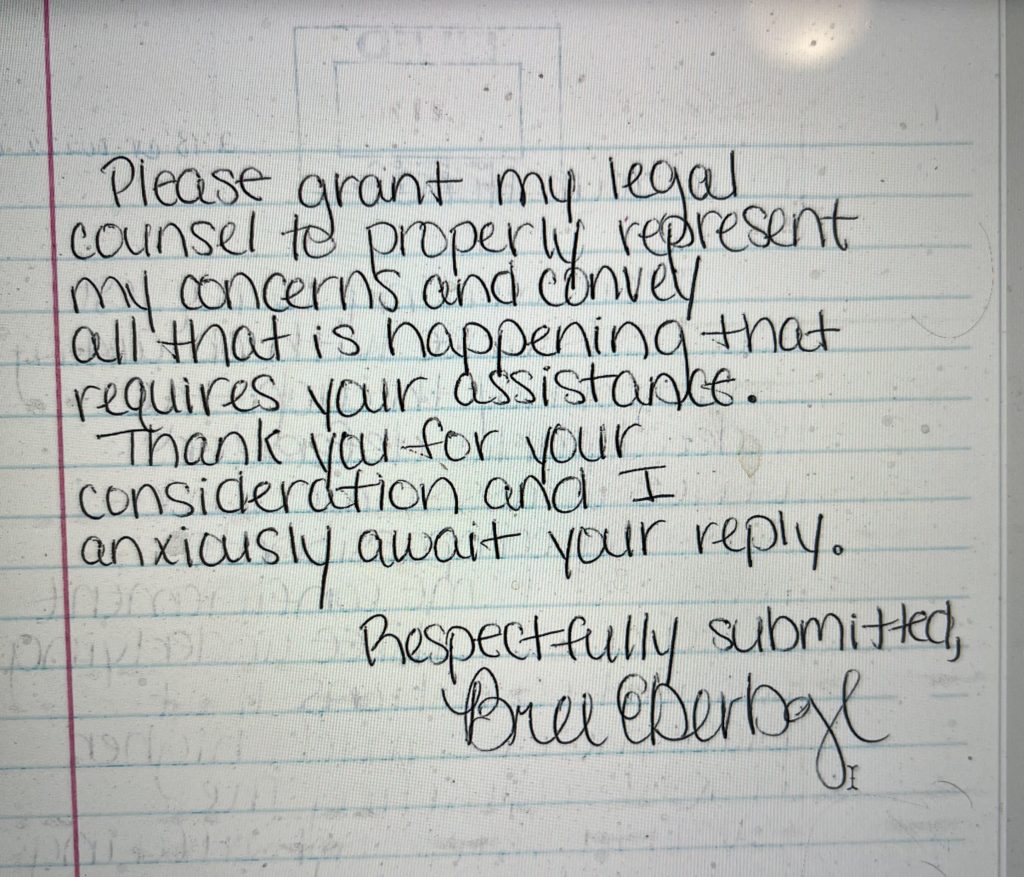
Please grant my legal counsel to properly represent my concerns and convey all that is happening that requires your assistance.
Thank you for your consideration and I anxiously await your reply.
Respectfully submitted,
Bree Eberbaugh”
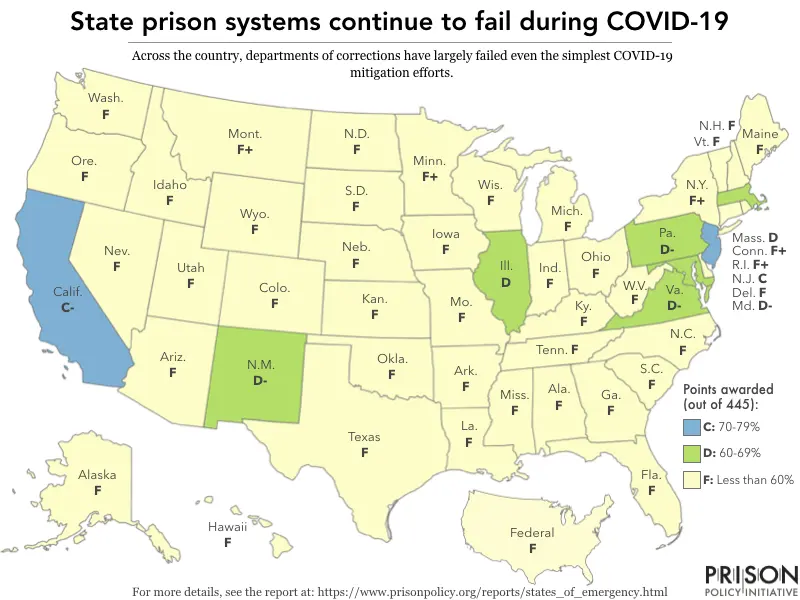
Incarcerated people in federal and state prisons are twice as likely to die of Covid as the general population. The situation in jails is presumed to be worse, but there’s no data as of yet. When the pandemic is over, will we recall Rebecca “Maria” Adams, Juanita Haynes, and Bree Eberbaugh, three women who asked for compassionate release that never came? Will we remember compassion itself?
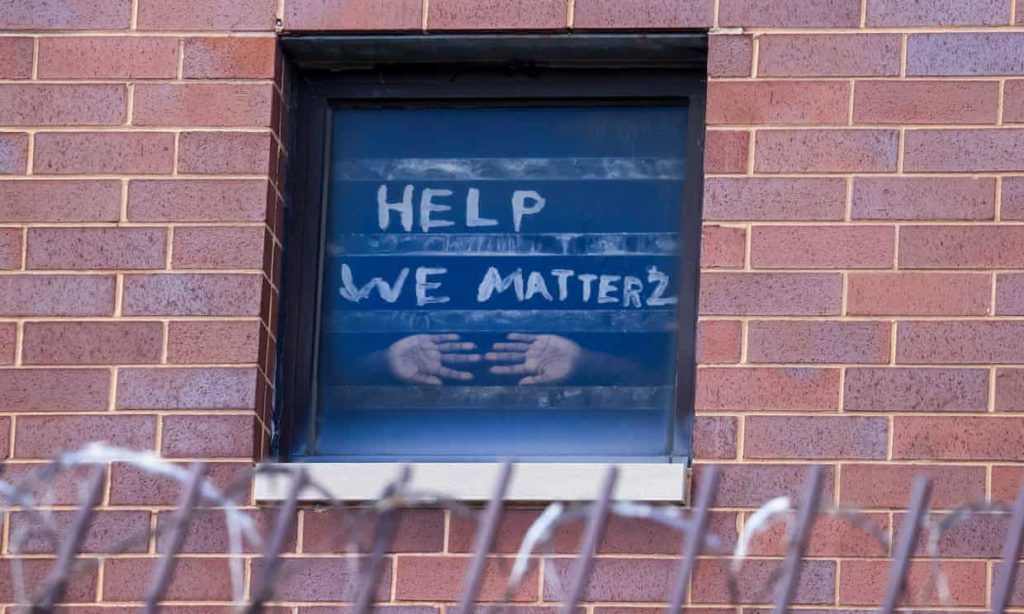
(Photo Credit: Kaiser Health News / LJ Dawson)